Reference :
V-P-GE-E-00610
Date :
09/02/2010
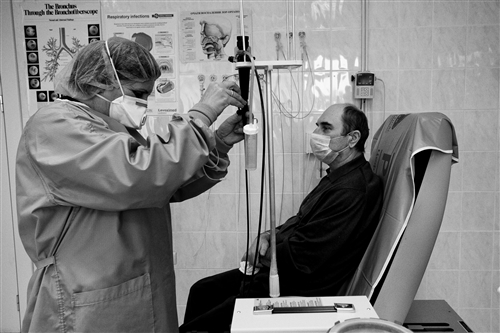
Caption :
Tbilissi hospital. A doctor uses a thin, flexible tube with a camera on the end to look for the source of bleeding in a patient’s lungs. The patient had no idea he was sick with tuberculosis until he started coughing up blood.
Confidentiality level :
public
Publication restrictions :
publication without restrictions
Description :
22-03-2010 Interview
Tuberculosis: stopping a killer that can't be kept behind bars
Tuberculosis, or TB, as it's commonly known, is a curable disease and yet it continues to spread across the globe. The vast majority of TB deaths are in the developing world but the airborne illness is also making a comeback in Europe and North America. The former Soviet Union is currently seeing some of the highest numbers of multi-drug resistant TB cases ever recorded. The ICRC's Nikoloz Sadradze has followed the situation in Georgia for many years and is now working with the authorities in Azerbaijan to stem the spread of TB in prisons. He warns that efforts must be stepped up to stop this deadly disease.
In general, why is TB spreading at such an alarming rate?
TB is an airborne disease. It spreads comparatively more easily than other infectious illnesses. You only need to inhale a small amount of bacilli to become infected. A lot of people may be shocked to realize that more than two billion people, or around one in three on the planet, carry the microbes that cause TB.
Luckily, only around one in 10 of those who have the bacilli will actually become sick in their lifetime. The microbes can lie dormant for weeks, years or even decades, waiting for the day when a person's immune system is down, for instance if they have to have chemotherapy or if they get the human immunodeficiency virus or diabetes. Then, TB can suddenly flare up and become life threatening as well as contagious.
If left untreated, each person with active TB will infect 10 to 15 other people per year, on average.
We hear about different types of TB, such as multi-drug resistant or extensively-drug resistant kinds. What's the difference?
Generally speaking, TB is a curable disease if people get the right medicine at the right time and stay on it. But it can be incurable as well. This is the case with extensively-drug resistant TB, or XDR-TB. There are some types of mycobacterium that can't be killed by antibiotics because they become resistant.
A lot of people think you can't catch drug-resistant TB right away. There's a common misconception that only people who stop taking their treatment wind up with multi-drug resistant TB, known as MD-RTB, or XDR-TB. In fact, you can catch either strain directly and then you wind up with the kind of TB that is very difficult to treat and cure. It's not a question of being a bad patient or getting a bad prescription... it's a question of bad luck.
Unfortunately, the number of drug resistant cases is on the rise in more and more places around the world, from Baku to Beijing and from Lima to London. According to the World Health Organization (WHO), as of last September, 57 countries had reported at least one XDR-TB case.
The Stop TB Partnership's slogan for World TB Day this year is "On the Move Against TB - Innovate to Accelerate Action". What gear would you say the international community is currently in when it comes to tackling this disease?
I think we're currently in third gear and we definitely need to step on the gas. We need to do more and move faster to put this disease higher on everybody's agenda in order to stop it from spreading further. It should be a public health priority in all countries, not just poor ones.
Illnesses like H1N1, Alzheimer's or heart disease often make the headlines but we don't see that much about TB. It's quietly stalking millions of people around the globe, yet there's no real sense of alarm. Why is that and what challenges do health professionals face in dealing with it?
It's a combination of a lot of things. First, there's a lack of awareness among the public and often, among decision-makers. It's also an incredibly difficult disease to treat. If you get regular TB, you're looking at being on medicine for six to eight months. You have to stay off alcohol, improve your diet and take a daily dose of medication. But this form is relatively cheap and easy to treat.
It's a different story if you catch a drug resistant strain, which requires a combination of pills, powders and jabs for 24 to 36 months or even longer, depending on how effective it is. It's very long, hard and expensive, sometimes costing tens of thousands of dollars. In Georgia and Azerbaijan, the authorities are footing the bill for treatment in the hope of getting it under control, but they still face many challenges.
It's been said that prisons, in particular, provide a perfect storm for TB to thrive and spread due to overcrowding, poor nutrition and a lack of health services. How are you tackling the spread of TB in Georgian and Azerbaijani jails?
Indeed, prisons are an ideal breeding ground for TB because of the close quarters. Prevalence in prisons is almost always higher than in the civilian population - sometimes 10 times more - owing to living conditions, nutrition and cross-contamination.
But while you can confine people to a cell, you can't keep TB behind bars. It spreads no matter what - whether it's the prison guard who catches it and takes it home to his unsuspecting family or the detainee who is released and finds it too difficult to stay on his medication once he's on the outside.
When the Soviet Union collapsed, so did medical infrastructures. As a result, ex-Soviet countries saw a sharp increase in TB cases and drug resistance during the 1990s. As part of our humanitarian work in countries affected by armed conflict, the ICRC visits prisons to monitor the conditions of detention. When we started visiting prisoners in Azerbaijan and Georgia in 1995, we discovered that TB was rampant among inmates, so we began working with the authorities to improve screening, treatment and follow-up.
How do you stop a killer that can't be kept behind bars?
Well, you start by making sure the right tools and resources are in place to identify and deal with the problem. In Georgia, we helped develop an early detection system and encouraged the implementation of the WHO's Directly Observed Treatment Short Course, or DOTS, strategy, which means patients have to take their medicine under medical supervision. As a result, more than 200,000 detainees were screened for TB between 1998 and 2009. Around 7,000 patients have been diagnosed with the disease and started treatment.
In addition, we made major improvements to 90 per cent of medical units in Georgia's prisons and penitentiary facilities, including the Ksani TB prison hospital near Tbilisi. The ICRC also constructed and equipped the TB National Reference Laboratory and helped train staff.
This month, we're handing over our detention-related TB activities to the Georgian authorities, but we'll continue to provide technical expertise and support.
What about Azerbaijan, which has seen a sharp increase in MDR-TB in recent years?
In Azerbaijan, we've been assisting prison authorities in carrying out an anti-TB programme for the past 15 years. Today, all prisoners in the country have access to modern diagnosis and high quality drugs, free-of-charge. As a result, the number of TB-related deaths at the country's Special Treatment Institution for prisoners near Baku plummeted from almost 300 in 1999 to 20 last year.
Almost three years ago, we supported the Ministry of Justice in implementing a pilot programme to treat MDR-TB patients. So far, over 220 prisoners have enrolled. We're also working with the Ministry of Health to provide MDR-TB treatment for people who have been released. We cover the transport expenses for the patients and provide them with food and hygiene items every month. There are currently 13 ex-detainees receiving treatment and I'm happy to report that another is now completely cured.
That said, while we've seen successes in terms of dealing with TB in a detention setting, Azerbaijan, like many other countries, still faces challenges in addressing it among civilian populations, from properly identifying new cases and ensuring access to treatment to tackling the stigma and isolation faced by many sufferers.
There's still a lot to be done in these areas, but I remain hopeful that with each passing year, the international community, aid agencies and local authorities will get one step closer to making TB a thing of the past, once and for all.
Original material :
digital
Resolution :
4000x2666
Orientation :
landscape
Colour/B&W :
black and white